Recovery Models and Frameworks
What Is Recovery?
Recovery means different things to different people and looks different for each person, with many factors involved.

Image description: brown background with blue text boxes, title is ‘recovery in mental health’. Other text ‘recovery means different things to different people and looks different for each person, with many factors involved.’ Under this is an image of a hard with hands and the following words scattered around: participation, context, process, hope, autonomy, culture, living well, supports and resources, meaning, social engagement, community, purpose, wellbeing, agency, identity.
Recovery is a process of living well, it is not a destination or a cure. It has been described as a transformation from a negative identity state to a positive state of psychological well-being (Dell, et al., 2021). It is about more than risk and symptom management (Read & Stoffel, 2019), is person-driven, relational, respectful, holistic, has many pathways, considers culture and addresses trauma (Substance Abuse and Mental Health Services Administration, SAMHSA, 2012). Enhancing recovery is an overall goal of the World Health Organisation’s (WHO) Mental Health Action Plan (2013). Key factors of recovery include: building hope, understanding strengths and weaknesses, planning for and engaging actively in occupations, having autonomy and agency, participation, identity, meaning, purpose, empowerment (Read & Stoffel, 2019; SAMHSA, 2012; WHO, 2013).
An early definition describes recovery as “a deeply, personal, unique process of changing one’s attitudes, values, feelings, goals, skills, and/or roles. It’s a way of living a satisfying, hopeful and contributing life even within the limitations caused by the illness” (Anthony, 1993, p. 15).
The recovery approach was adopted as the guiding principle for New Zealand’s mental health strategy and incorporated into the Mental Health Standards of 2001 (Gawaith & Abrams, 2006). A more recent shift in terminology places recovery within the larger concept of whanau ora and wellbeing for the whole population, including Māori models of wellbeing and the social determinants of health, with critiques of the recovery approach as too individualistic (O’Hagan, et al., 2012). The Mental Health Commission (2007) describes recovery in practice as: attitudinal change, listening and responding to service-user needs, service users in decision-making processes, closer liaison with family, strengths model, services that promote meaningful activities, social inclusion principles, and cultural appropriateness.

Recovery: A process of change through which individuals improve their health and wellness, live a self- directed life, and strive to reach their full potential.
4 Dimensions That Support Life in Recovery
Health
Home
Purpose
Community
10 Guiding Principles of Recovery: Person-driven, Many pathways, Peer support, Addresses trauma, Strengths/ Responsibility, Hope, Holistic, Relational, Culture, Respect
Image credit: SAMHSA (2012). SAMHSA’s Working Definition of Recovery. Retrieved from: https://store.samhsa.gov/sites/default/files/d7/priv/pep12-recdef.pdf
Image description: a circle shape containing the 10 guiding principles of recovery in different coloured wedges.
Recovery and Occupational Therapy
At the centre of occupational therapy is the idea that engagement in everyday, chosen and meaningful activities contributes to wellbeing. Promoting engagement in meaningful activities is a key component of the recovery approach in practice (Mental Health Commission, 2007) and “being occupied generates feelings of wellbeing, purpose, and meaning” (Cone & Wilson, 2012, p. 34). Cano-Prieto, et al. (2023) demonstrated that the number of meaningful activities a person is engaged in is strongly associated with aspects of personal recovery such as life satisfaction, resilience and hope. Engaging in purposeful activity such as exercise contributes to improved quality of life for people with severe mental illness (Alexandratos, et al., 2012), but it is important to note that satisfaction with everyday occupations was related to wellbeing for people with psychiatric disabilities, whereas activity level was not (Eklund & Tjörnstrand, 2020). So it is not solely the participation that is important, it is the satisfaction gained and the meaning of the activity that makes a difference for recovery.
Doroud et al. (2021) recommend that recovery-oriented practice uses co-production, provides opportunities for engagement in meaningful activities embedded into everyday life, and explores values and interests to support people to identify strategies to support recovery. Difficulties in daily life can lead to greater occupational dysfunction and in turn have a greater impact on the recovery process (Watanabe, et al., 2022), so focus also needs to be put on decreasing difficulties in daily life and improving occupational functioning to support recovery.

Figure 1.2. Goodness of fit: Recovery and AOTA practice framework. SAMHSA’s four dimensions of recovery support a life in recovery and can be used by occupational therapy practitioners to guide treatment planning and intervention decision-making (Read, & Stoffel, 2019).
Image description: screenshot from a textbook. Two blue arrows point towards each other. On the left the AOTA practice framework is listed: health through engagement in occupations; environments that support occupational choices; meaningful occupations; social participation and co-occupation. On the right the SAMHSA recovery dimensions are listed: health, home, purpose, community.
The above image demonstrates the fit between the American Occupational Therapy Association (AOTA) practice framework and the SAMHSA recovery dimensions (Read, & Stoffel, 2019). In the New Zealand context the ministry of health requires mental health service delivery to be in line with recovery principles. Cone and Wilson (2012) looked at occupational therapists’ use of the recovery approach and found that the recovery approach is difficult to distinguish from occupational therapy as engagement in daily occupations incorporates the recovery approach and the recovery approach is in line with occupational therapy beliefs and values about what contributes to wellbeing, with the core idea of occupational therapy being that engagement in meaningful occupations increases quality of life. Occupational therapists provided support with engaging in everyday experiences, practical things, linking to supports, getting out and doing, balancing activity and rest, finding motivation to get up, managing time use, choice, and worked with the whole person using recovery principles alongside other approaches (Cone & Wilson, 2012).
“Feelings of wellness when participating in occupations are linked to recovery values such as living with purpose and hope. Occupational therapists in this research used their professional knowledge to deliberately facilitate recovery, through engagement in everyday occupations.” (Cone & Wilson, 2012, pg.34)

Image description: a brown background with blue text boxes, heading ‘Recovery and Occupational Therapy’. A bidirectional arrow points sits between two statements ‘Occupational therapy promotes recovery’ and ‘Recovery promotes occupational performance’. Below this is a list: A recovery approach fits well within occupational therapy:
Person-centred practice, collaboration;
Hope, support, empowerment, building mastery;
Support for pursuing meaningful occupations and routines that promote health, well-being and balance;
Engagement across contexts (SAMHSA dimensions - health home, purpose, community);
1:1 interventions, groups, workplace and systems change, population level interventions.
In the bottom right is an image of two speech bubbles curled around each other.
Image description: brown background with blue text boxes, heading: ‘Personal vs Clinical Recovery’. In the first text box personal recovery is defined as: Living well. Leading a satisfying and meaningful life despite symptoms. Personal recovery does not necessarily correlate with symptom levels. It’s a unique and personal process, more subjective and process-oriented, sees the individual in context. An image of a person hugging themselves sits to the right. In the second text box clinical recovery is defined as Reduction of symptoms, improvement in functioning. Medical model view, objective and outcome focused, sees the individual as passive. An image of a clipboard and pen with medication sits to the left.
Recovery Frameworks
Outlined here: CHIME (Leamy, et al., 2011); Power-Threat-Meaning (Johnstone & Boyle, et al., 2018); SPICE (Vera San Juan, et al., 2021); Re-covery (Randal, et al., 2009).
CHIME (Leamy, et al., 2011)
Personal recovery is difficult to define because it is so individual. Leamy, et al. (2011) completed a systematic review and narrative synthesis to draw out common elements of personal recovery in mental illness. The resulting conceptual framework encapsulates five recovery processes, summarised using the acronym CHIME:
Connectedness,
Hope and optimism about the future,
Identity,
Meaning in life and
Empowerment
Two additional themes emerged from studies on recovery in black and ethnic minority populations:
Culturally specific facilitating factors
Collectivist notions of recovery
Subsequent scoping reviews support the dimensions of the CHIME framework (Van Weeghal, et al., 2019) and have found that measures of personal recovery are positively associated with the CHIME dimensions (Leendertse, et al., 2021). Sofouli (2020), notes that using the CHIME framework among cultural and ethnic minorities may need cultural adaptations to add spirituality and collective rather than individualistic ideas of recovery. Additionally, it is important to consider individual preferences, adapt the model to the population, focus on choice, risk taking, and learning to cope with challenges, use peer providers to enhance hope and empowerment, and focus on the process rather than the outcomes (Van Weeghal, et al., 2019).

Image credit: Progress in Mind
Image description: an infographic of the CHIME recovery framework. Each letter of the acronym goes across horizontally with a circular picture above each one. C - connectedness, picture of the world as a puzzle and two people putting the last piece in. H - hope, a picture of a blue sky and a person looking towards the horizon. I - identity, picture of a person looking at themselves in a mirror. M - meaning, picture of a person climbing a ladder above the clouds reaching for a star. E - empowerment, picture of a person with their arms crossed, ghost-like arms behind them are held up to each side showing strong muscles.
Power-Threat-Meaning Framework (Johnstone & Boyle, et al., 2018)
A framework for identifying broad patterns of distress and unusual experiences that incorporates social, psychological and biological factors, integrating existing models and practices. Views emotional distress and behaviours as understandable responses given a person’s history and circumstances, normalising these experiences, not pathologising them.
The framework asks the following questions as a way to explore validating narratives, meaning-making and increasing access to power and resources:
What has happened to you? (How is Power operating in your life?)
How did it affect you? (What kinds of Threats does this pose?)
What sense did you make of it? (What is the Meaning of these experiences to you?)
What did you have to do to survive? (What kinds of Threat Response have you used/experienced?)
What are your strengths? (What access to Power Resources do you have?)
What is your story? (How does all this fit together?)

Image credit: Juliet Young, Creative Clinical Psychologist
Image description: a cartoon style infographic of the Power Threat Meaning Framework with different aspects of the framework represented by 5 circles. Bidirectional arrows connect all of the circles. In the central circle the word ‘Power’ is in red text, the circle asks ‘how is/was power operating in your life?’ and lists examples of power: bodily, economic, legal, coercive, social capital, relational, idealogical. Top left circle: ‘Strengths’ in pink text, ‘what access to power resources do you have? e.g. solidarity, skills, support, access’ with a picture of two people hugging and heart and stars around them. Top right circle: ‘Threat’ in orange text, ‘how did/does it affect you? e.g. to emotional safety’ with a picture of an adult shouting and pointing at a child sitting with their knees drawn up to their chest. Bottom left circle: ‘Response’ in blue text, ‘what did/do you have to do to survive? e.g. learned to self harm to calm distress’, picture of a person looking sad. Bottom right circle: ‘Meaning’ in purple text, ‘what sense did/do you make of it? e.g. I felt excluded and ashamed’, picture of a person with their head bent forward and shoulders slumped.
SPICE (Vera San Juan, et al., 2021)
The SPICE framework was developed from a systematic review, focusing on lived experience perspectives. The authors noted the importance of expanding from just the personal perspective of recovery to include socio-political aspects as well as having user perspectives in service development and research. They found that
Service user definitions of recovery focused on social aspects, acceptance, connection
Caregivers focused on symptom remission and clinical definitions
Both groups mentioned being self-sufficient and achieving personal goals
Domains of the SPICE framework:
Social recovery - external approval and acceptance, trust, responsibility, meaningful relationships, role fulfilment (family and community), mutuality
Prosperity (legal, political and economic recovery) - expanding roles, empowerment, economic stability, availability of resources
Individual Recovery - individual goals, needs and responsibilities, everyday and meaningful activities, identity, future-focus, personal growth, sense of worth
Clinical Recovery Experiences - diagnosis, medication, symptoms, embracing or dropping labels, understanding of recovery, toolbox of strategies

Figure 2 [from original research article]. Meta-synthesis map. Visual representation of how the recovery paradigms and themes identified in this systematic review are related and their predominance in user/carer samples. The circles on left and right represent recovery as understood by users and carers, respectively. The outer circle presents recovery paradigms, while the inner circles refer to the themes and subthemes. The most prevalent themes are highlighted in bold letters.
Re-covery (Randal, et al., 2009)
A model of life, not illness, from a bio-socio-psycho-cultural-spiritual perspective.
Key concepts: normalising, respect, optimism, collaboration.
Components:
Map of the journey of re-covery - victorious or vicious spirals based on stressors and responses. Considers trauma, vulnerabilities/stress, maternal environment, genetics, patterns, triggers, early warning signs, consequences, sensations, feelings, thoughts, actions, spiritual context and how everything comes together to create cycles
Victorious cycles - hope-inducing, increase our strengths and decrease vulnerabilities, recognise patterns, identify early warning signs, develop skills to cope
Vicious cycles - spirit-breaking, strengths decrease and vulnerabilities increase, overwhelmed by triggers, side effects, risk behaviours
Building a bridge of trust - being with, cross the bridge of trust to the person’s reality, non-judgement, finding shared experiences and beliefs.
Mapping patterns, triggers and early warning signs - thoughts, feelings, sensations, behaviours, understand patterns and chains of events, identify strategies
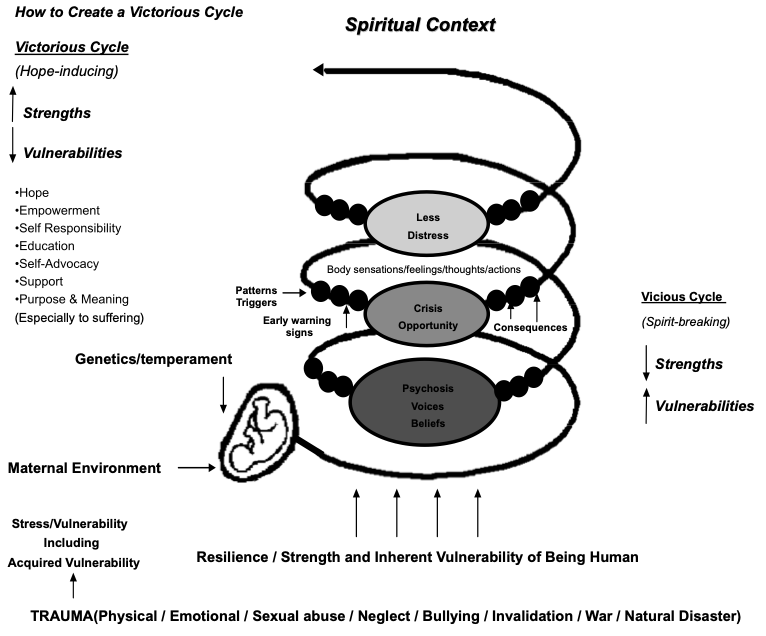
Figure 1. [From original research article] The Map of the Journey of Re-covery that forms a basis for explaining the Re-covery program.
Image description: An illustration of the Re-covery model with a picture of a baby in the womb and spirals leading upwards. At the bottom are the factors that contribute to the spirals with arrows pointing up.
So what can we do?
A recovery-based mental health system utilises community support, takes a broad view of the impact of mental illness, and assumes recovery is possible and non-linear (Anthony, 1993). Services need to listen and respond to people’s lived experience, work with people as equal partners, offer choices, use peer workers, and take a holistic approach (WHO, 2013).
Various documents describe recovery-oriented practice, including links between occupational therapy and recovery.
Mary O’Hagan (2001) outlined 10 competencies for mental health workers, highlighting personal resourcefulness, communication and relationships, promoting service user rights, partnerships and family/whānau participation.
Australia’s national framework for recovery-oriented mental health services focuses on promoting hope and optimism, being person first and holistic, supporting personal recovery, organisational commitment and workforce development, and action on social inclusion and the social determinants of health (Australian Health Ministers’ Advisory Council, 2013).
Engagement in occupations increases quality of life and links to recovery values such as purpose and hope (Cone & Wilson, 2012).
Participation in occupation promotes recovery and fosters a sense of purpose and meaning (Occupational Therapy New Zealand - Whakaora Ngangahau Aotearoa, OTNZ-WNA, 2016).
Australia’s national practice standards for the mental health workforce include recovery principles (Australian Health Ministers’ Advisory Council, nd; Victorian Government Department of Health, 2013). These are:
Uniqueness of the individual - individual at the centre of their care, supporting their strengths, encouraging them to take responsibility, considering impacts of trauma, discussing the importance of physical health and wellbeing, and including a carer’s experience where suitable.
Real choices - supporting positive risk taking while balancing duty of care, providing information for informed choices.
Attitudes and rights - respecting and promoting legal and human rights, conveying an attitude of respect and equal partnership, listening to and acting on communications.
Dignity and respect - being welcoming, creating a physically and emotionally safe environment, listening to and respecting the person.
Partnership and communication - working in partnership, client involvement in care planning, treatment and reviews, linking with other services, acknowledging each individual is an expert on their own life.
Evaluating recovery - utilising feedback, evaluating recovery outcomes regularly, measuring outcomes on a range of factors; training in recovery-oriented practice for clinicians, ongoing quality improvement.

Image description: a brown background with blue text boxes, heading ‘recovery-oriented services’. A bulleted list of points says: Responsive services - listen and respond to needs; Person-centred, strengths-based; Cultural responsivity and awareness, Respectful, relational, holistic; See recovery as more than risk and symptom management; Different pathways available; Support: hope, strengths and weaknesses, autonomy, agency, engagement, participation, identity, meaning; Peer support services available; See recovery within the larger context; Understand the social determinants of health. An image of a hand with outlines of people is in the top left and an image of a road with the words ‘together in recovery’ is in the bottom right.
Reflection points:
What are your takeaways about recovery?
What framework do you think would work best for you and your setting? Why?
What might this look like in your practice?
Where are you already using recovery principles and what would you like to change? How could you do this?
References
Alexandratos K, Barnett F & Thomas Y. (2012). The impact of exercise on the mental health and quality of life of people with severe mental illness: A critical review. British Journal of Occupational Therapy, 75(2), 48-60. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=amed&NEWS=N&AN=0152753
Anthony, W. A. (1993). Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosocial Rehabilitation Journal, 16(4), 11–23. https://doi.org/10.1037/h0095655
Australian Health Ministers’ Advisory Council (nd). Practitioners’ Guide to Recovery Principles. Retrieved October 6th 2023 from https://healthsciences.unimelb.edu.au/__data/assets/pdf_file/0009/3391344/Practitioners-Guide-to-Recovery-Principles.pdf
Australia Health Ministers’ Advisory Council (2013). A national framework for recovery-oriented mental health services: Guide for practitioners and providers. Retrieved October 6th 2023 from https://www.health.gov.au/sites/default/files/documents/2021/04/a-national-framework-for-recovery-oriented-mental-health-services-guide-for-practitioners-and-providers.pdf
Cano-Prieto, I., Prat-Vigué, G., Vilanova-Masana, R., Guillaume-Cornet, A., Giralt Palou, R., Lana-Francos, G., & Simó-Algado, S. (2023). Mosaic, an example of comprehensive and integrated social and health care: Care and practices oriented towards personal recovery. Frontiers in Health Services, 3. https://doi.org/10.3389/frhs.2023.1174594
Cone, E. & Wilson, L. (2012). A study of New Zealand occupational therapists’ use of the recovery approach. New Zealand Journal of Occupational Therapy, 59(2), 30–35.
Dell, N. A., Long, C., & Mancini, M. A. (2021). Models of Mental Health Recovery: An overview of systematic reviews and qualitative meta-syntheses. Psychiatric Rehabilitation Journal, 44(3), 238–253. https://doi.org/10.1037/prj0000444
Doroud, N., Fossey, E., Fortune, T., Brophy, L., & Mountford, L. (2021). A journey of living well: A participatory photovoice study exploring recovery and everyday activities with people experiencing mental illness. Journal of Mental Health, 31(2), 246–254. https://doi.org/10.1080/09638237.2021.1952950
Eklund, M., & Tjörnstrand, C. (2020). Associations between occupational and social interaction factors and well-being among people with psychiatric disabilities living in supported housing in Sweden. Journal of Occupational Science, 27(1), 54-68, DOI: 10.1080/14427591.2019.1620121
Gawith, L., & Abrams, P. (2006). Long journey to recovery for Kiwi Consumers: Recent developments in mental health policy and practice in New Zealand. Australian Psychologist, 41(2), 140–148. https://doi.org/10.1080/00050060600657988
Johnstone, L. & Boyle, M., et al. (2018). The Power Threat Meaning Framework: Overview. Leicester: British Psychological Society.
Leamy, M., Bird, V., Le Boutillier, C., Williams, J. and Slade, M. (2011), “Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis”, British Journal of Psychiatry, Vol. 199 No. 6, pp. 445-452.
Mental Health Commission (2007). Te Harerenga mo te Whakaōranga 1996-2006: The Journey of Recovery for the New Zealand Mental Health Sector. Retrieved from: https://www.moh.govt.nz/notebook/nbbooks.nsf/0/12912EA93B0B85EFCC2573C90068845D/$file/te_haererenga%20%201996-2006.pdf
Occupational Therapy New Zealand - Whakaora Ngangahau Aotearoa (2016). Occupational Therapists Working in Mental Health and Addictions Position Statement. Retrieved from: https://www.otnzwna.co.nz/wpfd_file/the-role-of-occupational-therapists-working-in-mental-health-and-addiction-position-statement/
O’Hagan, M. (2001). Recovery Competencies for New Zealand Mental Health Workers. Retrieved October 2nd 2023 from http://www.maryohagan.com/resources/Text_Files/Recovery%20Cometencies%20O%27Hagan.pdf
O'Hagan, M., Reynolds, P., & Smith, C. (2012). Recovery in New Zealand: An evolving concept? International Review of Psychiatry, 24(1), 56-63, DOI: 10.3109/09540261.2011.651447
Randal, P., et al. (2009) “The Re‐covery Model” – An integrative developmental stress–vulnerability–strengths approach to mental health, Psychosis, 1:2, 122-133, DOI: 10.1080/17522430902948167
Read, H., & Stoffel, V. (2019). Recovery. In Brown, C., Stoffel, V., & Munoz, J. P., (Eds.), Occupational Therapy in Mental Health: A Vision For Participation (2nd ed., pp. 3–13). F.A. Davis Co.
SAMHSA (2012). SAMHSA’s Working Definition of Recovery. Retrieved from: https://store.samhsa.gov/sites/default/files/d7/priv/pep12-recdef.pdf
Vera San Juan, N., Gronholm, P. C., Heslin, M., Lawrence, V., Bain, M., Okuma, A., & Evans-Lacko, S. (2021). Recovery from Severe Mental Health Problems: A Systematic Review of Service User and Informal Caregiver Perspectives. Frontiers in Psychiatry, 12, 712026. https://doi.org/10.1101/2021.05.13.21257172
Watanabe, A., Kawaguchi, T., Sakimoto, M., Oikawa, Y., Furuya, K., & Matsuoka, T. (2022). Occupational dysfunction as a mediator between recovery process and difficulties in daily life in severe and persistent mental illness: A Bayesian structural equation modeling approach. Occupational Therapy International, 2022, 1–11. https://doi.org/10.1155/2022/2661585
World Health Organisation (2013). Mental health action plan 2013-2020. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/89966/9789241506021_eng.pdf;jsessionid=E0D6D76D4B102F7BA82F6B550071EEAE?sequence=1